CPAP Alternatives: Sleep Apnea Treatments Beyond the Machine
CPAP works — but only if you actually wear it. The mask, the hose, the whistling leak at 3 a.m., the dry mouth, the partner who can't sleep through the noise: somewhere between 30 and 50% of patients walk away from CPAP within the first year, according to data published by the American Academy of Sleep Medicine. If you've tried it and tapped out, or you're avoiding a prescription entirely, you have real, evidence-backed sleep apnea and snoring treatment options.
At Michigan Nose & Sinus Health, Dr. J. Martin Ulrich evaluates the upper airway — nose, palate, and throat — to pinpoint why your airway collapses and which CPAP alternatives actually fit your anatomy. This guide walks through what works: oral appliances, nasal procedures, positional therapy, targeted surgery, and the lifestyle changes that move the needle.
Why CPAP Doesn't Work for Everyone
You're not failing therapy. The therapy is failing you.
Patients abandon CPAP for predictable reasons: mask discomfort and pressure sores, claustrophobia, air leaks that wake you up, a dry mouth that's worse than the snoring ever was, noise that disrupts your partner, and the hassle of traveling with a machine that needs power every night. For many, the deal-breaker is a blocked nose — pushing pressurized air into an obstructed airway feels less like therapy and more like suffocation.
The non-compliance numbers back up what patients already know. Peer-reviewed studies in the Journal of Clinical Sleep Medicine put long-term CPAP non-adherence between 30% and 60%, with roughly half of users stopping within the first 12 months.
Here's what often gets missed: most patients quit CPAP because the underlying anatomy was never addressed. A persistent nasal congestion problem, a deviated septum, or collapsed nasal valves make any positive-pressure therapy harder to tolerate — and they're fixable. An ENT-led evaluation looks at where the airway actually collapses. From there, the alternatives stop feeling like guesswork.
Understanding Your Sleep Apnea: Why the Right Alternative Depends on You
The right CPAP alternative depends on two things: how severe your apnea is, and where your airway collapses.
Severity, measured by your AHI (apnea-hypopnea index):
- Mild OSA (AHI 5–14): Most alternatives are on the table.
- Moderate OSA (AHI 15–29): Several alternatives, often used in combination.
- Severe OSA (AHI 30+): Fewer standalone options; combination therapy or surgery usually wins.
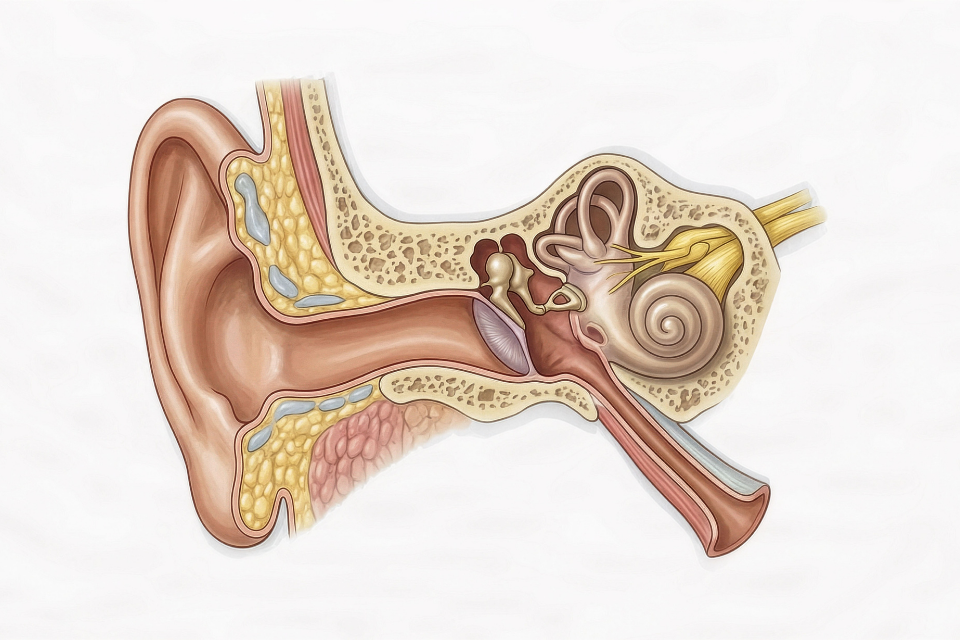
Site of obstruction matters even more. The airway can collapse at three levels: the nose (deviated septum, enlarged turbinates, nasal valve), the soft palate and uvula, or the tongue base. Many patients collapse at more than one level, which is why single-point treatments sometimes underwhelm.
Pinpointing where is the job of the evaluation. Dr. Ulrich uses in-office nasal endoscopy — and, when indicated, drug-induced sleep endoscopy (DISE) to observe the airway in a state mimicking real sleep. That's what separates a treatment that works from one that gets returned to the drawer.
CPAP vs. Top Alternatives at a Glance
- CPAP — Best for moderate to severe OSA. No invasiveness, but adherence is often low. At-home use.
- Oral appliance (MAD) — Best for mild to moderate OSA. No invasiveness. High adherence. At-home use.
- Nasal procedures — Best for nasal-driven OSA or CPAP intolerance. Minimal to low invasiveness. At-home after recovery.
- Soft palate surgery — Best for palatal collapse. Moderate invasiveness. Permanent.
- Positional therapy — Best for position-dependent OSA. No invasiveness. Moderate adherence. At-home use.
A proper ENT evaluation tells you which row applies to you.
Oral Appliance Therapy
A custom-fit dental device worn during sleep — most often a mandibular advancement device (MAD) — that nudges the lower jaw forward and opens space behind the tongue. For the right patient, it works quietly, fits in a travel bag, and doesn't plug into a wall.
Who it's best for:
- Mild to moderate OSA
- Patients who can't tolerate CPAP
- Frequent travelers
- Snorers without confirmed apnea
What to expect: A dentist trained in dental sleep medicine takes impressions and custom-fits the device. Over 2–4 weeks, the jaw position gets titrated until you hit the sweet spot between comfort and effectiveness. A follow-up sleep study — often at-home — confirms the device is actually dropping your AHI. Periodic check-ins catch bite changes early.
The trade-offs: Oral appliances are quiet, portable, and have higher long-term adherence than CPAP. The downsides are real but usually mild: jaw soreness in the first few weeks, occasional bite shifts over time, and reduced effectiveness in severe OSA.
Dr. Ulrich coordinates with local dental sleep medicine providers and uses your sleep study results to verify the appliance is hitting its target — not just feeling like it is.
Treating Nasal Obstruction: The ENT Difference
A blocked nose forces mouth breathing, which collapses the airway and makes CPAP — or any alternative — work harder. For many patients, opening the nose is the highest-leverage move in the entire treatment plan.
Here's the chain reaction: when you can't breathe through your nose, your mouth falls open during sleep, the tongue and soft palate drop backward, and negative pressure in the airway spikes with every inhale. That's the exact mechanical setup for apnea events. It's also why nasal airway obstruction drives sleep disturbances that patients often blame on something else entirely.
This is where an ENT evaluation separates itself from a sleep lab alone. Dr. Ulrich treats the structural causes directly:
- Septoplasty. A septoplasty corrects a deviated septum to restore balanced airflow. For some patients, it's the difference between tolerating CPAP and abandoning it. For others, it's what makes avoiding CPAP possible in the first place. If you've ever wondered whether correcting a deviated septum would improve your breathing, the answer for severe deviations is usually yes.
- Turbinate reduction. Shrinks enlarged turbinates that block airflow. Quick recovery, often done alongside septoplasty in the same visit.
- Balloon sinuplasty. Performed in-office under local anesthesia. Not a direct apnea treatment, but opening chronically inflamed sinuses reduces the nighttime congestion that worsens snoring and apnea.
- Nasal valve evaluation. When the sidewalls of the nose collapse on inhalation, targeted treatment of the valve restores airflow — something CPAP cannot fix.
For some patients, fixing the nose alone drops AHI meaningfully. For others, it's the step that makes the next treatment finally work.
Positional Therapy
Some patients only have apnea events while sleeping on their back. If a sleep study confirms position-dependent OSA, training yourself to stay off your back can meaningfully drop your AHI — sometimes enough to avoid other treatment entirely.
The options range from high-tech to almost comically simple:
- Positional pillows or wedges that keep you on your side
- Wearable vibration devices that buzz when you roll supine
- The tennis ball trick — a tennis ball sewn into the back of a t-shirt. Low-tech, zero cost, and genuinely effective for the right patient.
Positional therapy is often combined with another treatment rather than used alone. A sleep study is the prerequisite: without confirmation that your events are position-dependent, you're guessing.
Surgical Options When Other Treatments Aren't Enough
When conservative treatments fall short, surgery addresses the structural cause of airway collapse. The right procedure depends entirely on where the airway gives way — which is why a thorough workup of surgical and non-surgical pathways comes before any scheduling conversation.
Soft palate procedures. Radiofrequency ablation (RFA) stiffens floppy palate tissue in an outpatient setting with quick recovery. The Pillar procedure places small implants in the soft palate to reduce vibration and collapse. Both work well for snoring and mild palate-driven apnea.
UPPP (uvulopalatopharyngoplasty). Removes excess tissue from the soft palate, uvula, and throat. More invasive, typically reserved for moderate-to-severe palate collapse after careful patient selection. The recovery is real, and Dr. Ulrich talks candidly about whether the trade-off makes sense for each patient.
Tongue base procedures. For tongue-driven collapse identified on endoscopy. Several techniques exist; the right one depends on anatomy.
Combination (multilevel) surgery. The airway often collapses at more than one level — palate and tongue base, or nose and palate. Multilevel procedures address each site in a coordinated plan, often pairing septoplasty or turbinate reduction with the main apnea surgery in a single operation. Success hinges on identifying the exact sites of obstruction up front. A single-procedure surgery aimed at the wrong level is how patients end up disappointed.
Frequently Asked Questions
Can mild sleep apnea be treated without CPAP? Yes. Mild OSA often responds well to oral appliances, positional therapy, weight loss, and treating underlying nasal obstruction — alone or in combination.
What is the best alternative to CPAP? For most mild-to-moderate cases, an oral appliance has the strongest evidence and the highest adherence. For nasal-driven apnea, opening the nose is the highest-leverage step. For severe palate or tongue collapse, surgery is often the most durable option.
Will fixing my deviated septum cure sleep apnea? Not always — but it can meaningfully reduce severity, eliminate snoring, and is often the difference between a patient who tolerates further treatment and one who quits.
Is untreated sleep apnea actually dangerous? Yes. Untreated OSA is linked to high blood pressure, stroke, atrial fibrillation, type 2 diabetes, and daytime driving accidents. The goal isn't any single treatment — it's finding one you'll actually use.
Better Sleep Without the Mask
CPAP isn't the only path to treating sleep apnea — and for many patients, it isn't the right one. Oral appliances, nasal procedures, positional therapy, and targeted surgery all work when matched to your airway, your severity, and your life.
If CPAP failed you, scared you, or you want a second opinion before starting, schedule an evaluation with Dr. J. Martin Ulrich at Michigan Nose & Sinus Health. Better sleep is possible without a mask.
Schedule a Sleep Evaluation — (810) 695-3766

Balloon Sinuplasty vs. Endoscopic Sinus Surgery — Choosing the Right Procedure for Chronic Sinusitis